
Our Programmes
Sentinelles offers immediate and staunch support, and advocates a holistic approach that takes into account the specific medical, psychosocial, educational and economic situation of each person.
Individualised monitoring enables them to access their fundamental rights while rigorous support helps them achieve independence.
Although operational contexts are quite different, the proposed overall approach remains the same, i.e. differentiated and sustainable support.
Health focus
Sentinelles’ programmes aim to improve the medical and social conditions of children and adults. Our interventions include a care component ranging from medical and social monitoring to surgical missions, depending on the situation. The common thread of these services is to offer tailor-made support that takes into account the individuality and uniqueness of each person we support.
Find out about the different aspects of our actions:
Local care: Medical and social care aims to provide care in our reception centres. This aftercare can last several months or years depending on the situation.
Medico-social aftercare: Medico-social aftercare is systematically carried out with everyone, children and adults, that we support. Visits to the villages and families by our local teams aim to provide long-term aftercare and improve the families’ living conditions.
Surgical care: Surgical procedures are sometimes necessary. Children and adults who need surgery are operated on during surgical missions (co-organised by local partners, in neighbouring countries or during medical transfers to Switzerland, specifically for noma).
Awareness-raising and prevention: We are committed to participating in the early detection of symptoms, as in the “Noma” or “Women and Girls with Obstetric Fistulas” programmes. To this end, awareness-raising and training activities are carried out with the community, village authorities, health workers, public health students and NGO staff.
Education focus
Education focus
In all of our programmes, we provide access to education and training to develop the recipients’ independence, whether they are children, young people or adults. We are convinced that schooling, education and training are one of the main keys – if not the key – to developing both communities and individuals.
Social reintegration focus
Social reintegration focus
The aim of this component is to ensure family and social aftercare for each child and adult we support. To carry out this task, our teams of social workers go directly to the places where the families live or, in our programmes in the DRC and Madagascar, regularly visit people in prison. In this way, we provide aftercare and prepare for their reintegration into society. Access to certain regions is difficult due to the poor state of the roads and the deteriorating security situation (banditry, risk of attack and kidnapping). The social workers maintain a constant link with the children and their families from the moment they are admitted to the moment their case is closed.
Economic strengthening focus
Economic strengthening focus
Our actions support the economic situation of families so that they become fully independent. We draw on the skills and experience of the recipients of the support to help them develop an income-generating activity (IGA) or undertake training. For example, workshops are regularly offered to mothers of children in our centre in Colombia to help them become self-sufficient or to mothers of children with noma to improve their knowledge of nutrition and hygiene.
Care in Switzerland









Sentinelles organises the transfer of children and young adults to Switzerland, when medical care is not possible in their country of origin. Children and young adults with noma or other facial diseases undergo consultations and operations at the Geneva University Hospitals or during surgical missions organised with our local partners. In Switzerland, they are hosted in Massongex, at “La Maison” belonging to the Terre des hommes Valais.
The plight: Children suffering from serious pathologies may be left untreated by parents and families without resources in all of the countries where we are active. This is particularly the case for children with noma.
What we know: Reconstructive surgery requires considerable technical and human resources. It allows children to have a well-structured face again and includes plastic, reconstructive and aesthetic surgery, as well as maxillofacial surgery.
Transfers
In order to offer the best possible support and stay to patients, transfers are carefully prepared. To this end, we request a complete medical and social file beforehand, so that we know the child, his or her state of health, daily life and family environment as well as possible. Our local staff prepare the children and their families for the trip and also take care of the administrative aspects.
At Sentinelles’ head office
The programme manager coordinates and manages the transfer: planning the surgical programme in consultation with the surgical teams, booking the plane ticket, finding a companion from Aviation Sans Frontières (ASF) for the trip and, if necessary, an interpreter, planning the stay in the quarantine section of the hospital in Rennaz and finally requesting accommodation at the Terre des hommes House in Massongex. Once the patient is in Switzerland, the head of the programme establishes the link between the hospital and the host accommodation, coordinates the care, accompanies the child to the medical consultations, takes care of the administrative procedures and manages a team of volunteers to organise visits to the patient in hospital.
Once the patients arrive, it is important to spend time with them in order to get to know them, put them at their ease, and explain the next steps.
The hosts accommodation
Sentinelles’ patients are hosted in Massongex, at “La Maison”, belonging to the Terre des hommes Valais, which meets all the necessary requirements, both medically and in terms of overall care. Many children and young people go there to take part in activities such as school, creative workshops, games, cooking and walks.
As of 1 July 2015, “ La Maison” has granted Sentinelles free healthcare. Patients also receive follow-up physical therapy if needed.
Other Assistance
This programme aims to support people who are alone, who sometimes have not received treatment, with no solution to their problems, totally destitute and unable to take care of themselves or their loved ones.
Algeria : 1 family
Support for a family where the father was very seriously injured during a demonstration when he was a teenager. Throughout his working life, his very limited vision and kidney problems have meant he has only been able to do odd jobs with insufficient income to feed his family.
Russia : 1 young woman
Medical support for a young woman who became a paraplegic at the age of 12 following a failed back operation, and who is now in good health despite her disability. Devoted donors and friends continue to support her and her mother with the purchase of expensive medical equipment and with her specific needs.
Nepal : 1 young man
Support for a young man who was hosted in the Sentinelles reception centre in Kathmandu in 1999 because of kidney problems that could not be treated in his village. He is the only young person in Nepal monitored by Sentinelles, which continues to support him to meet the needs related to his kidney failure; his condition still requires medical supervision and very expensive medication. We are currently seeking direct support from a pharmaceutical company to cover the medical costs.
Syria :
Sentinelles continues to work with the association Vivere to provide care and legal support to young Syrian women who have been unjustly imprisoned for years in the regime’s jails. We also provide vital nutritional support to some 60 babies whose mothers are unable to breastfeed.
Facts & Figures
Facts and figures in 2021 for the “Other Assistance” programme
Work team
In Lausanne : 1 part-time volunteer staff member
Children with noma














The plight :
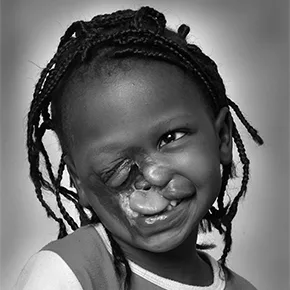
Noma was present in the West until the beginning of the 20th century. It mainly affects children between the ages of 2 and 6. It is fatal in 70 to 90% of cases and leaves deep scars on the survivors.
Noma is an infectious disease that begins with a benign lesion in the mouth. It develops rapidly: in a few days or weeks, without treatment, the children die in 70 to 90% of cases. If they survive, they suffer terrible aftereffects, as the disease profoundly disfigures their face and often causes the jaws to be locked in a closed position (constriction). In addition to the physical aftereffects, there is also psychological suffering, as the disease is often experienced as a curse or fate, leading to marginalisation and a feeling of shame for the children and their families.
Distress: Present in the West until the beginning of the 20th century, noma mainly affects children aged 2 to 6. Deadly in 70 to 90% of cases, it leaves deep scars on the survivors.Noma is an infectious disease that starts with a benign lesion in the mouth. Its evolution is lightning: in a few days or weeks, without care, the child dies in 70 to 90% of cases. If he survives, he keeps terrible after-effects, deeply mutilating his face, often causing a total blocking of the jaws in closed position (constriction). In addition to the physical after-effects, there is also psychological suffering, as the disease is often seen as a curse or fate, leading to marginalization and feelings of shame for the child and his family.
What we know : The cause of noma is still unexplained; however, malnutrition, poor oral hygiene and an immune system weakened by other diseases are risk factors for the development of noma. Early detection, followed by the administration of a simple antibiotic treatment can stop the progression of the disease and cure a child in 2 to 3 weeks.
Local care :
Noma support consists of providing treatment and care in our reception centres in Ouagadougou and Zinder. The state of health of the children in our centres requires aftercare that can last several months or even years.
Medical and social aftercare :
Medical and social aftercare is routinely carried out with all children cured of noma in our centres. Visits to their villages ensure they are integrated socially and educationally and improve their families’ living conditions.
Surgical treatment :
Reconstructive surgery is offered to children with serious aftereffects. They are operated on during surgical missions organised by partners in-country, in neighbouring countries or during medical transfers to Switzerland.
Awareness-raising :
We organise awareness-raising among the population and community actors to prevent and detect noma at an early stage. Traditional authorities, health workers, public health students and NGO staff are targeted by these awareness-raising and training sessions.
Care for children



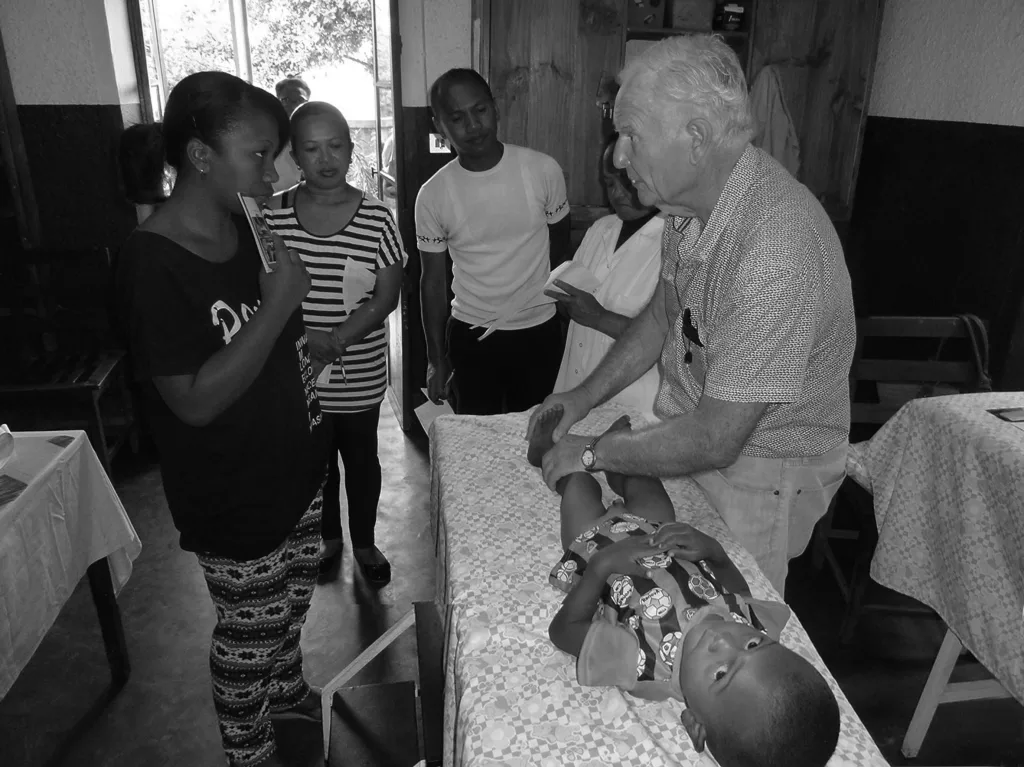













The plight : Children with serious illnesses are deprived of care because their families do not have sufficient resources for their treatment.
What is know : Due to economic and geographical barriers in particular, access to health care is not guaranteed. Many children from poor families with serious illnesses, burns, heart disease, disabilities or disfigurement are left without care due to a lack of resources. Sentinelles facilitates their access to health services.
Local care
After a thorough social investigation, Sentinelles ensures that the children are medically and surgically cared for, and prioritises local medical and surgical treatment. Depending on the options available, care is provided by local health professionals or during surgical missions in all the countries in which we are active.
Aftercare
When a child receives treatment, their medical and social care continues in the home for as long as the situation requires. Once the child has recovered, we ensure that they attend school or receive vocational training.
Awareness-raising and prevention
Our teams organise various awareness-raising and prevention activities for health professionals, the general public and civil and religious authorities.
Find out more about these different activities through our programmes.
Girls and Women in extremely vulnerable situations



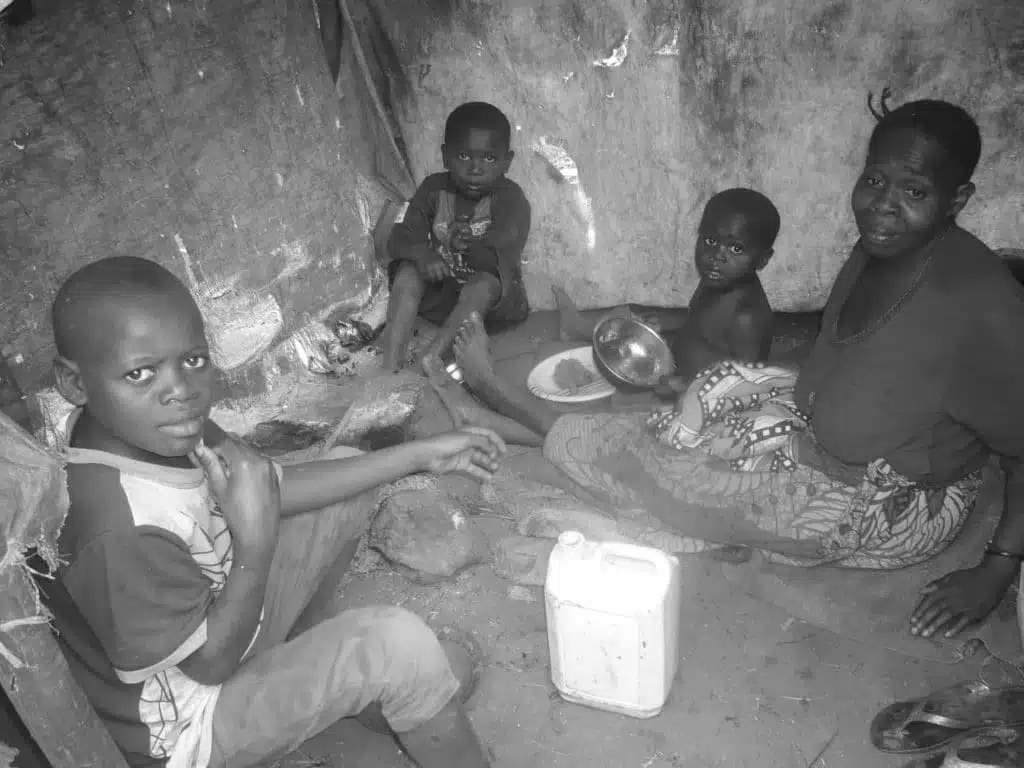






The Plight: The country’s extreme poverty has destroyed solidarity and prompted many men to abandon their families, leaving behind women and children, sometimes born as a result of rape. Feeding them becomes a daily challenge and the only means of subsistence for these mothers is to offer their labour for an often miserable income. Physically and morally broken, they struggle for their survival and that of their children. Others are imprisoned with their children, most often for crimes related to their living conditions.
What is know: he women that Sentinelles supports live in extreme poverty in a rural area within a radius of about sixty kilometres of the city of Bukavu in South Kivu. The implementation of income-generating activities (IGAs) enables them gradually to meet their families’ needs.
Activities in the Democratic Republic of Congo
health and social care component
Individual care, which is always geared towards the independence of families in the medium or long term, includes medical care and psychological support, occasional food support, housing assistance (design, renovation and/or reconstruction of huts), income-generating activities, education for children and vocational training for young people who have completed their schooling or who have never attended school.
Social component in prisons
The particularly disastrous situation of the inmates in Bukavu’s central prison led us to launch a nutritional, medical and social support programme for women and their children during their imprisonment, as well as reintegration assistance upon their release. To this end, Sentinelles provides individual and group psychological support, training workshops and social services. The children have access to education or benefit from socio-educational activities in the nursery we have set up (project supported by La Chaîne du Bonheur (Swiss Solidarity)).
Women and girls with obstetric fistulas









The plight : Obstetric fistulas are mainly caused by prolonged labour, sometimes lasting several days, without medical assistance, or when a caesarean section is performed too late. They can also be the result of genital mutilation and early marriage. Vesicovaginal fistulas (VVF) and/or rectovaginal fistulas (RVF) are lesions of the bladder, urethra, ureters, vagina and sometimes the rectum that cause continuous or intermittent leakage of urine and/or stools.
What is know: In most cases, the child dies and the woman suffers permanent incontinence. A woman suffering from fistulas will not automatically go to a health centre; she will hide her problem by living in isolation and sometimes in shame. Many people believe that there is no cure for this “disease” and view it as a punishment. Women with fistulas are often rejected by their husbands and by the community. They live on the margins of society and this also affects their economic situation, even though they can be cured.
Local care
Our reception centre in Ouagadougou for children with noma also accommodates women and their companions during the post-operative period, for one month or more depending on the case.
Surgical treatment
Sentinelles supports women to access VVF/VRF surgery and receive medical and psychological support throughout their stay in hospital and the post-operative period, until they have recovered.
Social component
During their convalescence at our reception centre, the women have access to training such as cooking, soapmaking, or managing a small business, with a view to setting up income-generating activities (IGAs) that will facilitate their social, family and economic reintegration. They also attend hygiene and nutrition awareness sessions. At the end of the medical supervision, if the woman is declared cured, she takes away a kit that will enable her to start an IGA.
Awareness-raising and prevention
The programme to combat obstetric fistulas aims to break the taboo by raising general awareness, primarily in villages, Health and Social Promotion Centres (CSPSs) and Medical Centres (CMAs), where possible. Our staff members try to remove the negative beliefs associated with this disease. The testimony of a woman who has recovered from fistulas is often sought and is effective for prevention. These awareness-raising and prevention campaigns are also carried out through screenings of the film “Dagouba’s fistula”, which are attended by hundreds of people per session, and through messages on prevention and detection of obstetric fistulas broadcast on community radio stations.
Child protection















The plight: Mining, and in particular coalmining, is the main resource in the region of Amaga, in the department of Antioquia. Despite government action to legalise mines and protect miners, this activity remains partly informal. The lack of compliance with employment legislation, accidents and economic instability cause serious social problems for families in the region, which is also plagued by violence linked to micro-trafficking of drugs and the presence of criminal gangs. Some children are abused or neglected and their basic rights are not respected. Their mothers themselves face serious financial and psychosocial difficulties.
What is know: Our Home is the only reception facility in the region and provides a caring and professional environment for children and adolescents in serious difficulty. Our objectives are to offer them psychological and medical support, guarantee their fundamental rights, socialise them and recreate and/or strengthen the parent-child relationship. The work also extends to their families, to help them return to a supportive environment.
Some children in the coalmining region in the south-west of the department of Antoquia are in situations where they are abused or their rights are violated in their family and social environment. The living conditions of vulnerable mothers and families are sometimes also seriously affected.
Fighting sexual abuse:
The vast majority of both girls and boys at the Home have been abused by someone close to them. The psychologist from the Lucerito Foundation, one of Sentinelles’ partners, monitors children suffering from trauma and provides individual and/or group therapy on a regular basis and in a safe environment to support children and their mothers/families.
Individual assistance:
We support and monitor children in their environment and ensure they receive frequent visits where they are growing up. Individual assistance can also take the form of support and guidance in administrative procedures or in vocational guidance and job-seeking.
Talibé children


The plight: Talibé children are entrusted by their parents to a Quranic teacher (marabout), the head of a daara (Quranic school), so that he can take charge of their religious education. Once in a daara, the child becomes a talibé and lives in the daara under the full responsibility of the marabout, who holds all rights over him or her.
What is know: Talibé children are mostly boys between the ages of 5 and 15, from poor, often rural families. In exchange for their integration into the daara and their education, talibés have to perform domestic work and are usually forced to beg on the streets in order to support themselves, the marabout and his family. They are sometimes subjected to severe corporal punishment and neglect.
Local monitoring
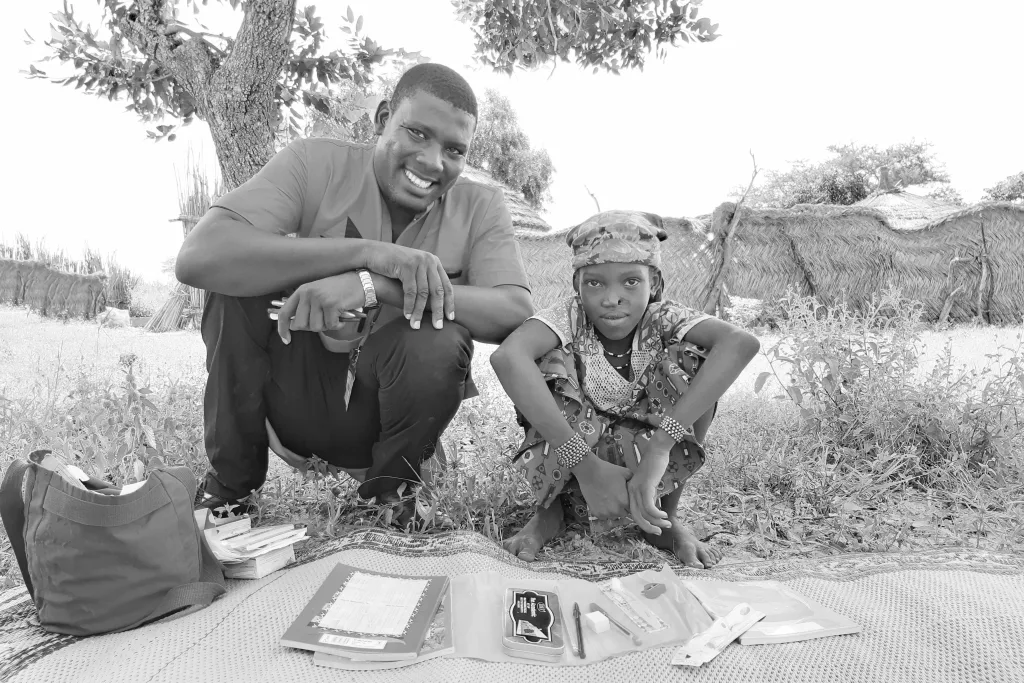
Sentinelles carries out its activities in several daaras in Mbour (region in western Senegal), offering marabouts support for medical monitoring as well as for the talibés’ schooling or literacy. To promote a sustainable approach, Sentinelles is developing market gardening and livestock projects, so that the marabouts can provide care and education for the talibés through their own efforts. We also work in collaboration with various actors in the community to enable them to become involved in monitoring the welfare of the children. The neighbours, the neighbourhood representatives, the neighbourhood elders (badjenu gokh), the daara mothers, the health centres, etc are all involved in monitoring the talibés. This helps keep attention focused on the talibés’ living conditions in the longer term, even after Sentinelles has left.
Awareness-raisnig and prevention
In parallel with the activities in different daaras, Sentinelles organises campaigns to raise awareness of abuse and, if it occurs, reports the person or people responsible to the competent authorities. For talibé children who are victims of violence, Sentinelles puts medical and/or social monitoring in place. Once their care has finished, we set up a social, educational and academic project in their families. Quarterly visits are carried out to ensure that their circumstances are improving.
Child prisoners
Children, big boys, big girls, in prison or in detention or “reeducation” centres. A few weeks, months or years. Forgotten or punished. Serious offences, minor misdemeanours, or nothing at all. But sentences that are often heavy and long. They are there because they have nowhere else to go.
In prison, feed them more, give them medical treatment, love them more. Listen to them, get to know them, gain their confidence. And work towards their freedom.
Outside, take them in and slowly, patiently, teach them how to live and from what. By giving them the means. Do all that we can so that they do not fall back into the same misfortune.
Guide children for the blind
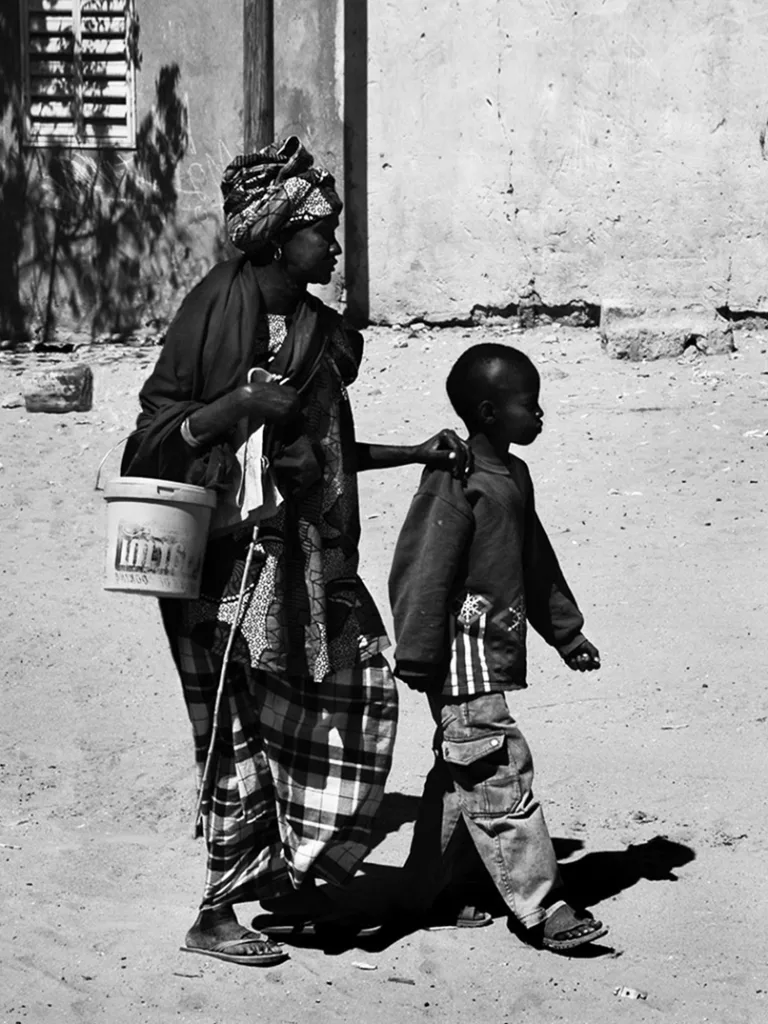

The plight: Children as young as three or four years old from families where one or both parents are blind are forced to take care of them and find ways to access basic necessities for themselves and their families. They are often living in very insecure circumstances, but, as the name of the programme suggests, become “guides for the blind”, and accompany their parents to beg in the streets.
What is know: This situation prevents them from attending school, deprives them of a carefree childhood and sometimes leads them into delinquency.
Action on the ground
Sentinelles offers tailor-made support, sometimes long-term, to ensure a lasting improvement in the living conditions of beneficiaries and their families through the implementation of income-generating activities.
Action and awareness-raising
Individual monitoring of child guides for the blind in terms of education, training, medical care and social integration are set up during home visits, always in close collaboration with families. Some of the particularly vulnerable families receive temporary food aid.
Food support
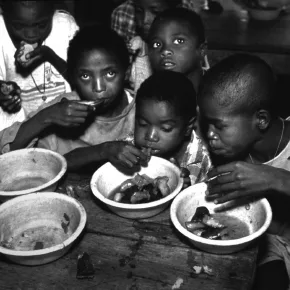
We ensure the right to food through the social aspects of each of our programmes. Depending on their needs, we refer children to nutritional recovery centres or offer them food support alongside income-generating activities, with a view to fostering their independence.
Food support








Food belongs to everyone, but people die of hunger in their millions. If the planet’s development plans Through the social components of each of our programs, we ensure the right to food. Depending on the needs, we direct the children to nutritional recovery centers or offer them food support while developing income-generating activities, with a view to their autonomy.
Burkina Faso
Burkina Faso in figures:
Population: more than 20 million inhabitants
Fertility rate: 5.2 births per woman
Infant mortality rate (before age 5): 76 per thousand
Literacy rate of 15 to 24 year olds: 47% for men and 33% for women
In 2020, the UNDP ranking ranked Burkina Faso 182nd out of 189 countries, according to the Human Development Index (HDI). While the country has “moved up” one place in the ranking since 2015, more than 40% of its population still lives below the poverty line. According to the provisional results of the latest census, the country has a population of 20.5 million. The population growth rate of 3.1% per year remains among the highest in the world with an average of 5.2 children per woman and an estimated life expectancy of 56.7 years. The proportion of children aged zero to fifteen is estimated at 47.4 per cent and that of children under five at 18.1 per cent.
Mothers and children are the most vulnerable population groups. In 2015, only 66% of births were attended by a qualified health professional. The maternal mortality rate of 371 deaths of women during pregnancy, childbirth or within six weeks of birth per 100,000 births and the average birth rate among girls aged 15 to 19 of 132 per 1,000 women are among the highest in the world.
According to the 2020 nutrition survey, nearly 10% of the population suffers from acute malnutrition (9.1%) and a quarter of the population from chronic malnutrition (24.9 %). The regions most affected by malnutrition remain the Sahel, Centre-North and East. In Burkina Faso, more than a third of under-five deaths are directly or indirectly attributable to malnutrition. The assessment of the nutritional status of women of reproductive age is also worrying with a high prevalence of acute malnutrition of 4.1% according to upper-arm circumference and 9.0% according to body mass index.
The security situation has continued to deteriorate in recent years due to the presence of radical armed groups in the Sahel region, particularly in Burkina Faso, with an increasing impact on the population. According to OCHA, in comparison with the previous 10 years, 2020 was the most challenging year in terms of the humanitarian situation. Difficult conditions had built up for already vulnerable populations: insecurity, conflict between communities, food and nutritional insecurity, floods and strong winds, COVID-19 and the accompanying restrictive measures. The number of internally displaced persons (IDPs) in Burkina Faso increased from 614,000 in January 2020 to 1.074 million IDPs on 31 December 2020, an increase of 75%, and to more than 1,368,164 in July 2021. The trend of closing health facilities or operating them at a minimum level remained almost the same throughout 2020, with an average of 1 million people consistently deprived of access to health care. The same trend was also observed in the closure of schools due to violence: as of 5 December 2020, the government figure stood at 2,169 schools closed, affecting 306,946 students. The results of the Harmonised Framework exercise of November 2020 showed that, at national level, 2.02 million people were currently in food crisis with a projection of 2.86 million people (June to August 2021).
Faits & Chiffres
Facts and figures in 2020 for the Noma program in Burkina Faso
Sentinelles assisted 204 children, adolescents and adults, including
- 85 children, adolescents and adults with noma
- 56 newborns and children with cleft lip and palate
- 58 children and adults with osteitis (bone infection), tumors, burns and other facial conditions
- 5 children and youth with heart disease
- 3 new cases were opened during the year and 10 cases were closed, of which 2 were lost to follow-up and 8 completed their medical/social follow-up.
In 2020 – Sentinelles sensitized 323 health workers in 153 health and social promotion centers (CSPS)
Work teams
In Ouagadougou and Fada N’Gourma: 12 local collaborators
- 1 local manager for the noma and FVV/FRV programs (until October: 1 local manager per program)
- 1 administrative assistant, 2 nurses, 1 social worker, 2 animators, 1 driver, 2 cooks, 2 guards in Ouagadougou (and until October: 2 guards in Fada).
In Lausanne: 4 collaborators
- 1 person in charge of the noma and FVV/FRV programs at 100%.
- 2 volunteers
- 1 staff member of the Child Care Program and 1 staff member of the Relief Program for children affected by noma in Niger work in close collaboration with this program.
Expenditures in 2020
CHF 231’504
Program facts and figures Women with obstetric fistula
Sentinelles assisted 111 women who were followed through the various stages of their care
- 10 women were screened: 5 with vesico-vaginal fistula (VVF) or recto-vaginal fistula (RVF) and 5 with prolapse; they were given an individual file
- 9 women were operated and accompanied during an operative mission.
- 5 of them suffered from DVF/VRF and 4 from prolapse
- 15 women benefited from postoperative follow-ups
- 2 women who underwent urinary diversion between 2004 and 2016 were followed up
- 8 women were declared cured and their medical file closed
- 28 women benefited from social follow-up and the setting up of income-generating activities
- 55 women are waiting for an intervention at the end of 2020
Work teams
In Ouagadougou and Fada N’Gourma: 12 local employees
- 1 local manager for the noma and FVV/FRV programs
- 1 administrative assistant, 2 nurses, 1 social worker, 2 facilitator, 1 driver, 2 cooks, 2 guards in Ouagadougou
In Lausanne: 4 employees
- 1 full-time noma and FVV/FRV programs manager
- 2 volunteers
- 1 employee from the Child Care Programme and 1 employee from the Relief Programme for children with Noma in Niger work in closely with this programme.
Expenditures in 2020
CHF 231’504
Our Partners
Medical centers – Hospitals in Burkina Faso
- Yalgado Ouedraogo University Hospital (CHUYO),
- Persis Pediatric Medical Center,
- Schiphra Protestant Medical Center,
- Ouagadougou Center for Recovery and Nutritional Education (CREN),
- Morija
- Regional Hospital Center (CHR) of Fada N’Gourma
- Bethany Medical Center of Fada N’Gourma
- Numerous CMAs and CSPSs in the eastern and central regions
Associations and other organizations
- Association Persis Valais and Persis Burkina
- Bilaadga
- FAMOG
- Hymn to the Children Foundation
- Charles de Gaulle Hospital
- La Chaîne de l’Espoir, France
- La Voix du Paysan, Radio Manedga, Radio Salaki
- Secours Dentaire Burkina Faso (SDBF),
- Ouagadougou Financial facilities + technical partnership
- Swiss Cooperation Agency and Swiss Consulate in Ouagadougou.
- Association Ensemble pour Eux (EPE)
- Physionoma Association
- Saint Camille Hospital of Ouagadougou, Dr. Moussa Guiro
Colombia
Located in the extreme northwest of South America, Colombia connects Central America (Panama) with South America (Peru, Brazil, Ecuador and Venezuela) and has access to the Pacific and Caribbean coasts. The country has a population of 50 million inhabitants in a territory covering one million km2, concentrated on the coasts and in the Andes, especially in the five major cities: Bogotá, Medellín, Cali, Barranquilla and Cartagena.
Economically, Colombia is growing, although inequalities persist. The unemployment rate is 13%. A large part of the country makes its living in the informal economy and, according to DANE (Colombia’s National Administrative Department of Statistics), 40% of the population lives in poverty.
The country’s history is marked by violence: political assassinations, coups d’état, the formation of self-defence groups, military juntas. In 1948, the assassination of Gaitán led to 10 years of violence between the left-leaning Liberal Party and the Right-leaning Conservative party.
This period saw the birth of the debate about the distribution, sharing and use of land, an issue that continues to this day. The violence was aggravated by cocaine and arms trafficking in the 1980s and 1990s. The various cartels control entire regions, while right-wing self-defence militias control others. This violence flourishes in the poorest areas of the country, where half the population lives in extreme poverty. The cartels control the entire production chain, from the cultivation of the plant (coca) to its export to consumer countries. Currently, about 70% of the cocaine sold in the world comes from Colombia.
In 2016, following 50 years of civil war, a peace agreement between the government and the communist guerrilla group FARC was finalised. Five years after the signing of the agreement, crucial points remain unresolved (rural reform, socio-economic reintegration of ex-guerrillas, substitution of illicit crops, reconciliation and reparation to victims).
Local context of action
Sentinelles is active in the Andean region of the southwestern department of Antioquia, where job opportunities are scarce. Without access to education, the possibility of engaging in any activity other than coalmining is very low. This context of poverty and violence motivates Sentinelles to support abandoned and severely abused children and women by offering them tailored assistance that promotes dialogue, trust and commitment.
Sentinelles rescued 76 children, adolescents and adults, including :
The relief and support component: in the Amagá – Minas shelter
- 22 children and their families received care and psycho-social follow-up
- 3 children in a day care center
- 3 children with serious learning difficulties participated in the state school reinforcement program
- 2 young girls have benefited from a psychiatric follow-up
Care for victims of sexual abuse
- 4 girls benefited from therapy
The component: Individual assistance
- 20 families received regular support in their living environment (9 children, 8 young adults and 13 adults)
Support to families during the Covid-19 crisis
- 68 families were supported, representing approximately 400 people
- 26 families were supported outside the program in March and April
Work teams
In Minas (Antioquia) :
- 7 local staff, an intern ans an occasional professional accountant
In Lausanne :
- 1 programme manager at 60%.
Expenditure in 2021
CHF 134’125
Our partners
- Lucerito Foundation
- Passion & Heart Foundation
- National Apprenticeship Service – SENA
- AIESEC Organization
- Federation of NGOs of Antioquia
- Hogar Juvenil Campesino y Minero de Amagá (Amagá Peasant and Mining Youth Home)
- Fondation Patronato
- New Era
Democratic Republic of the Congo
Africa’s second largest country, the Democratic Republic of Congo, straddles the equator in Central Africa. It is home to an estimated 86 million people and covers an area of 2,345,000 km2.
The country is ranked 179th out of 189 nations on the UNDP Human Development Index. According to World Bank data, approximately 64% of the population lives below the poverty line.
For more than 20 years, the eastern part of the Democratic Republic of Congo has been under attack by armed gangs of all kinds, in particular the Interhamwe, a genocidal group from Rwanda that settled in the forests of South Kivu at the end of the 1994 genocide. Villages are looted and burned, men are massacred and women are raped and subjected to many forms of torture. This is known as rape as a weapon of war.
Although the conflict is officially over, insecurity persists, particularly in the north-east and in South Kivu province, which are areas favoured by armed gangs because of their mineral-rich subsoil and international mine sites.
Many men flee poverty to look for work in the mines, deserting their families. Many die there because of a lack of medical care or are killed by the armed gangs operating in the region; others return home empty-handed, sometimes ill, and unable to provide for their families. In this extremely unfavourable security, economic and social context, women find themselves abandoned with their children and unable to provide for their families.
Faits & Chiffres
Facts and figures 2020 of the “Women victims of violence, abandoned with their children” program
Sentinelles rescued 571 people, including:
The social component
- 63 families received direct support, i.e. approximately 383 people
- 13 homes under construction/full or partial rehabilitation
- 188 children enrolled in school
- 13 young people received professional training
- 5 families became independent after several years of support.
Women detained at the Bukavu central prison and their children
In April 2020, the support program for women detained at the Bukavu central prison and their children began. All of them receive nutritional, medical and social support during their incarceration, as well as reintegration assistance upon their release. The children also benefit from schooling or regular follow-up in the prison kindergarten by our specialized social worker. This project is supported by La Chaine du Bonheur.
The social aspect: in prison
- 58 inmates and 8 children received direct support
- 5 children attending school
- 23 children outside prison, from families of incarcerated women
- 2 young girls in vocational training
- 2 women received support for reintegration.
Work team
In Congo: 5 local collaborators
- 1 administrator
- 3 social assistants
- 1 driver
In Lausanne: 1 collaborator
- 1 program manager at 40%.
Expenses in 2020: CHF 133’599
Our Partners
- Chaîne du Bonheur
- Vivere Association
- International Organization V-Day (City of Joy, Bukavu)
- Foyer Ek’ Abana (Archdiocese of Bukavu)
- Association Un seul but (Marin, Neuchâtel)
- Don Bosco Bukavu
- Mamas for Africa
- APEC (Psychosocio-educational action in favor of children and adults in conflict with the law)
Madagascar
Madagascar is the fifth largest island in the world and a southern Africa island state located in the Indian Ocean and separated from the mainland by the Mozambique Channel. It covers an area of more than 587,000 km2. The country is ranked 164 out of 189 in the UNDP’s latest Human Development Index (HDI) update, and is therefore dealing with extreme structural poverty. Its population is estimated at 26.9 million, 75% of whom live on less than PPP $1.90 (purchasing power parity) per day.
The serious political crisis that the country experienced from 2009 onwards led to a reduction in foreign investment and development funds from the usual donors, the closure of many businesses and, as a result, increased the impoverishment of a very large section of the population.
The return of both constitutional order and international partners took place in 2014 with the election of Hery Rajaonarimampianina. He was controversial throughout his term in office, and failed to solve the country’s difficulties. He was defeated in the first round of the 2018 presidential election by the two former heads of state who were the main players in the 2009 crisis. Andry Rajoelina has been country’s leader again since January 2019. Since then, his power has been considerably strengthened with the election of his supporters at local and parliamentary levels, as well as in other institutions.
Although the national economy has recovered following this return to order and a peaceful transition, the living conditions of the majority of the Malagasy people were still extremely insecure before the coronavirus pandemic. With the pandemic, they have become much worse.
More than a quarter of school-age children do not attend school, roads are not maintained, health, water and electricity systems are inadequate, and the security situation is appalling; all of these factors act as a brake on the country’s development. Access to sufficient food, water, health care, education and housing remains very difficult. The reality of many children and adolescents is determined by illiteracy, low levels of education, insecure employment in the informal economy, social and family breakdown and delinquency. Young girls, women and their children are particularly vulnerable in this situation and are its first casualties. The country has an extremely high number of single-parent families. In many cases, single mothers are left with no means of providing for their families.
Facts and figures on socio-medical follow-up actions
Sentinelles has helped more than 540 people (more than 2’700 people have benefited from our actions) in the framework of our different programs
Work team
In Madagascar: 43 local staff
2 coordinators, 4 social workers in charge of the program, 11 social workers, 3 educators, 2 doctors, 1 physiotherapist, 6 animators and trainers, 1 teacher, 1 lawyer, 2 housekeepers, 1 secretary, 1 accountant, 1 micro-credit agent, 2 drivers, 3 guards, 2 deputy guards
In Lausanne: 4 collaborators
- 1 program manager (80%)
- 1 part-time administrative assistant
- 1 part-time volunteer accountant.
Expenses in 2020
CHF 357’235
Childcare component
- 72 children from 70 families benefited from the care program
- 8 children underwent surgery, 2 children had deformities that were treated with a cast
- 30 children were followed in rehabilitation at the Sentinelles physiotherapy office. The regularity of physical therapy sessions at our office was disrupted for several months due to the health situation. To reduce the risk of regression, our physiotherapist provided families with exercises to practice at home
- 29 new devices were provided including 15 pairs of reinforced or orthopedic shoes
- 61 children were weighed, 64 benefited from the nutritional recovery program. Of these, 13 were integrated because they were more or less severely malnourished. The others had to reach the ideal weight to undergo or recover from surgery
- 92 children and young people benefited from school assistance
- 5 young people and mothers received vocational training
- 4 new economic aid projects (microcredits) were launched
- 57 family members benefited from specialized medical follow-up. There were 8 hospitalizations
- 32 families in precarious situations received temporary food support
- 11 cases were closed
This program was funded by the Gertrude Hirzel Foundation since May 1, 2019; it continued until the end of April 2020.
Right to be component
- 24 families, most of them large, living in severe poverty, were followed; they all received food, medical and psychosocial support. 8 families in the process of becoming autonomous still benefited from school assistance only
- 17 people benefited from specialized medical follow-up, including 1 psychological. There were 7 hospitalizations
- 46 children benefited from school assistance, including 7 in boarding school
- 11 people received vocational training, of which 5 were boarders
- 2 new economic aid projects (microcredits) were launched
- 1 housing assistance was granted
- 17 families in precarious situations received temporary food support
- 1 case was closed.
Dispensary of Antohomadinika
- 1,409 families (6,616 people) were enrolled in the dispensary’s health insurance scheme
- 1’862 people, including 853 children, consulted the dispensary and received medical care
- Usually more than 1’000 women take part in the family planning program; unfortunately this year a shortage of contraceptive products prevented this activity
- 34 women attended prenatal consultations and 38 newborns were examined in postnatal consultations
- 18 children were monitored for weight. The nutritional recovery program for these children was provided by Action contre la Faim
- Due to the health situation, the traditional consultation days given in a nearby crèche (Oasis) could not take place. There were no home visits.
- Four health education sessions were held, two of which were on Covid 19. The vaccination campaigns against poliomyelitis, in collaboration with the Ministry of Health, could not be organized because of the health context related to Covid 19.
The reception house
Several families stayed there for several days to several months. 41 children, young people and women stayed there for health reasons, training, protection measures or while waiting for a durable solution. During the vacation periods, the young people placed in boarding school, for lack of other places to stay, came to recharge their batteries and took part in the various activities set up.
The training workshop in Ambohidahy
- 15 people followed the sewing, knitting and cooking courses
- 16 families followed the individualized management course in order to launch an income generating activity
Small Courses
During the 2019-2020 school year, 20 children and youth attended support or refresher courses, 5 of them were only transient. Of the 15 students who were regular, 4 were able to be integrated into the public school, 3 are in training; 4 are continuing the course and 4 withdrew
Le Petit Cours could not operate during the few months of school closure decreed by the Government. Despite this, the results were judged globally satisfactory by our teacher.
Social and medical services, home visits and general information
- 3’365 medical consultations
- The shortage of contraceptive products prevented the implementation of the family planning program
- 88 children were placed under weight watch, including 20 malnourished children who entered our nutritional recovery program. Our doctor judged the results of this program to be good but insufficient. The consequences of the situation caused by the pandemic are mentioned as the main reasons for this observation (absenteeism)
- More than 42 tons of food products, more than 18’000 pieces of soap, more than 14 tons of charcoal and 203 blankets were sold for children in nutritional recovery, families under food support, the shelter, the prison and the students of the training workshops and the Sentinelles’ Petit Cours
- 3 weeks of awareness campaigns and health prevention were carried out by our doctors. 5 other awareness sessions, including 2 on covid 19, were carried out.
- 260 days of social permanence were carried out in our premises
- 752 visits were made to families for their psychosocial follow-up; more than 29,680 km were covered.
Social and family reintegration component
Rehabilitation Center of Anjanamasina Mandrasoa (CRM) – (young boys)
In the Center
- 85 boys were taken care of; all of them benefited from the socio-educational and cultural activities set up by Sentinelles
- 36 social days at the Center
- 2,107 trips to the court for investigation or hearing, all of which were taken care of by Sentinelles; 191 young people were released (some were taken care of by Sentinelles only at the time of their release)
- 103 somatic examinations were conducted outside the Centre.
We were unable to operate within the MRC for 5 months, from April to August, due to health restrictions related to Covid 19.
Outside the Center
- 150 released youth and their families received psychosocial follow-up
- 213 children received (or are still receiving) school assistance. (Among them, 34 are young people who have passed through the rehabilitation center and 166 are part of their siblings; 23 of them are studying in boarding schools)
- 38 young people have taken (or are still taking) vocational training, 17 of whom are in boarding school
- 16 youth have already entered the world of work through vocational training, an income-generating activity or a starter kit
- 8 new economic aid projects (microcredits) have been launched
- 20 families benefited from housing assistance. Among these, 7 houses were built or repaired, 3 rent subsidies and 10 equipment and material subsidies (furniture, mattresses, utensils, etc.)
- 91 families in precarious situations have benefited from temporary food support, as well as 23 young people in boarding schools
- 16 children and 2 mothers followed the nutritional recovery program
- 2 people received specialized medical follow-up, 3 received neurological follow-up and 3 people were hospitalized
- 4 suppletive judgement procedures in order to obtain birth certificates have been launched and are still in progress.
- 43 files were closed this year.
Antanimora Central Prison (Underage girls, pregnant women and women incarcerated with their children)
In the prison
- 20 underage girls at the time of their incarceration, including 10 new entrants, were followed up; all of them received food, medical and material support, follow-up of their legal situation and took part in socio-educational, cultural and training activities set up by Sentinelles. 9 of them went to court and 11 were released
- 1 child of an incarcerated minor girl was taken care of and welcomed in our kindergarten (see below)
- 24 days of social permanence for the girls were carried out within the prison
- 9 sensitization sessions on different themes were held
- 60 medical consultations by our doctor
- 2 girls benefited from a pregnancy follow-up. They gave birth after their release.
Outside the prison
- 43 girls and their families were followed up outside the prison
- 44 children benefited from school assistance
- 2 young people received vocational training
- 7 families in precarious situations received temporary food support and 9 children followed the nutritional recovery program
- 2 people benefited from a specialized medical follow-up
- 3 new economic aid projects (microcredits) were launched
- 21 cases were closed
Children incarcerated with their mothers and pregnant women
In the prison
- 48 mothers with their 48 children, 34 pregnant women and their 16 newborns, as well as 5 other children of inmates who have had a short stay were taken care of
- 70 children were welcomed in the kindergarten. Those over 18 months of age who were to be released according to the law were taken in by their families or placed in an appropriate structure. Among them, 22 were taken in by the Sisters of Saint-Maurice in their center located near the prison
- 27 days of social permanence for women were carried out
- 82 mothers participated in the Sentinelles training workshop
- 9 sensitization sessions on different themes were held
- 705 medical consultations for children and women in the prison and 22 dental consultations. 53 children were weighed, 1 of them was put on nutritional recovery. 2 children were hospitalized
- 28 incarcerated pregnant women received prenatal follow-up (6 of them gave birth in the maternity ward of a hospital in the capital during their detention; they were then given postnatal follow-up in the prison)
Outside the prison
- 64 mothers and their families were monitored
- 52 children received school assistance, 18 of them in boarding schools
- 4 young family members or mothers received professional training
- 15 new economic aid projects (microcredits) were launched
- 10 housing aids were granted to as many families
- 38 families in precarious situations received temporary food support and 17 children followed the nutritional recovery program
- 8 people received specialized medical follow-up. There were 12 hospitalizations
- 21 cases were closed
The “Tovovavy Mendrika” component: children and young girls who have been sexually assaulted
- 2 girls who have been sexually assaulted have benefited from a solid psychosocial follow-up according to their specific needs. 2 other girls whose psychosocial follow-up is completed and whose families are in the process of becoming autonomous still benefited from our support for the schooling of their children only
- 9 girls and/or members of their siblings have benefited from school assistance, including 4 in boarding school
- 2 families in precarious situations received temporary food support and 2 children followed the nutritional recovery program.
Niger
Niger is a West African country thirty times the size of Switzerland, with a population of around 24 million people, and is located in the Sahel belt, with no access to the sea. Three-quarters of the country is in the desert zone.
Every year, the country ranks at the bottom of the Human Development Indicators, making it one of the poorest countries in the world. 80% of the population depends on agriculture, only one in four people is literate and the school enrolment rate is one of the lowest in the world. In 2020, extreme poverty affected more than 10 million people, i.e. more than 40% of the population. Food insecurity, a weak health system and low levels of education are just some of the factors contributing to endemic poverty.
Niger’s economy depends mainly on agriculture, and so is increasingly affected by climate change, which not only greatly reduces agricultural yields but also causes extreme weather events such as floods and droughts.
Although there appear to be few direct victims of the Covid-19 pandemic, the indirect consequences of the pandemic are a further severe blow to a country whose growth rate fell sharply between 2019 and 2020.
Major insecurity problems in both the east and the west have increased since 2015 with the presence and proliferation of jihadist groups in the Sahel. The country is regularly the scene of attacks and massacres against security forces and civilians. This weakens the economy and the population and undermines national security.
As a preferred transit area for migrants from sub-Saharan Africa, Niger is currently home to large refugee camps and internally displaced persons.
Faits & Chiffres
Facts and figures in 2020 from the “Noma” program in Niger
Sentinelles rescued 300 children who were followed through the different stages of their care
The care component: the reception center
- 60 new children with noma were taken care of by our teams
- 29 children with noma were fully treated and their reintegration assured (files closed)
- 28 people on average stayed at the center each month (min: 11 in April, max: 37 in February, August and October)
- 183 consultations for screening and/or treatment of gingivitis, acute necrotizing gingivitis, thrush and candidiasis prevented possible cases of noma
The care component: surgical missions
- 18 children with noma were operated on
- 2 children were presented in surgical consultation in anticipation of complex management
- 2 children who were to be transferred to Switzerland in 2020 could not be transferred because of Covid-19. Their transfer is postponed to 2021
- 1 surgical mission was carried out with 2 partners (Hilfsaktion Noma e.V., Interplast Germany e.V.)
The prevention and awareness component
- 7’286 targeted people were sensitized in 241 localities in rural and urban areas (2’498 villagers, 3’814 religious representatives, 459 matrons, 233 village chiefs, 272 health workers, 10 teachers) attended these sessions;
- 310 students from 3 health schools were trained in early detection, management and prevention of noma
- 45 NGO staff members were sensitized to noma detection and prevention
- 272 health workers from more than 200 health facilities were trained in early detection, management and prevention of noma;
- 2 radio awareness spots were created to be broadcast widely by community radios to raise awareness among local populations
- 269 children suffering from gingivitis were detected during awareness sessions in villages or neighborhoods
Social component: follow-up in the bush
- 730 visits in the bush were made during the year
- 351 households received support from Sentinelles: 95 of them received food aid, which represents more than 15 tons of millet, the staple food in Niger;
- 147 children were monitored in their schooling;
- 6 young people received vocational training assistance;
- 1 four-week vacation course organized by Sentinelles brought together 25 children (school support), 4 young people (vocational training) and 3 teachers to supervise them and encourage them to continue their schooling or training;
- 15 families of noma victims received economic assistance to develop an income-generating activity in order to become independent.
Work team
In Niger: 21 local collaborators
- 1 field coordinator
- 1 administrative assistant
- 3 persons in charge of the care, awareness and social components
- 3 qualified nurses
- 2 social assistants
- 1 animator
- 3 drivers
- 2 cooks
- 2 stewards
- 3 guards
In Lausanne: 2 employees
- 1 program manager (100%)
- 1 employee of the “Childcare” program in close connection with this program
Expenses in 2020
CHF 311’570
Our Partners
- Human Appeal International (HAI).
- Niger-Amitié.
- Association Au Coeur du Niger: schooling of children victims of noma in the association’s boarding school in Zinder.
- Yara LNC Association, GRYK boarding school, Zinder
- Bucco-Dental Center of Zinder
Senegal
Senegal is a West African country with a population of more than 16 million people, half of whom are under 20 years of age. It was ranked 168th out of 189 in 2019 by the UNDP, with a human development index of 0.512, and, like the other countries in the sub-Saharan zone, is one of the countries with low human development.
Independent since 1960, the Republic of Senegal, which has been led since 2012 by President Macky Sall, has achieved a certain balance and remains one of the more stable countries in Africa. However, it operates at two speeds, and there are still very pronounced disparities between urban and rural areas. Although access to health services is among the best in West Africa, life expectancy is still only 63 years.
Unpredictable rainfall is always capable of hampering agricultural production, while shocks in neighbouring countries (Ebola epidemic, increased insecurity in Mali and the wider region) might result in a slowdown in tourism, trade and transport in Senegal. The poverty rate has reached 46% according to the latest estimates.
Despite considerable efforts in terms of education budgets, only 69% of children are enrolled in primary school and many children do not have access to it.
Quranic education still dominates as the sole source of education. School is compulsory and has to be paid for, which means that many parents in disadvantaged regions entrust their children to a marabout, sometimes from the age of four. In the daara, they will receive a religious education, and will also learn humility, respect, perseverance and how to live in a community. However, the worsening of the economic context and the emergence of a large number of fraudulent and exploitative marabouts, mean that the living conditions of these children have become extremely challenging, especially in urban areas. Without access to health care and education, and in most cases forced to beg in order to feed themselves, they risk beatings and sometimes serious abuse if they do not bring a certain amount of money back to the marabout every day.
Although Senegal ratified the International Convention on the Rights of the Child (CRC) in 1991 and enacted the law of 29 April 2005 against begging relating to “the fight against the trafficking of persons and similar practices and the protection of victims of trafficking” these laws and conventions are still not applied. According to the Partnership for the Rescue and Reintegration of Street Children (PARRER) and Human Rights Watch, between 50,000 and 76,000 children beg throughout Senegal.
Care for children:
A lot of children come from poor families, and so are uncared for, because of a lack of resources.
Sentinelles takes on the care of children suffering from serious diseases, injuries, burns, or heart conditions, and children who are disabled or disfigured, following a thorough social investigation. They are then treated in Senegal, within the limits of available resources. In order to empower the family, a financial contribution is requested, however small, when the family is able to provide it.
We always prioritise treatment carried out locally by competent surgeons, or during surgical missions organised by Sentinelles or its partners.
However, wherever possible, children who cannot be operated on in Senegal, and who are sometimes at risk of death, are transferred to Switzerland, in close collaboration with the specialists and hospitals concerned (through the “Soins en Suisse” (“Care in Switzerland”) programme).
When children are under our care, their medical and social monitoring continue in their homes for as long as the situation requires. Once the children have recovered, we ensure that they can go to school or take up vocational training.
However, children who cannot be operated on in Senegal, and who are sometimes in danger of dying, will be transferred to Switzerland when possible, in close collaboration with the specialists and hospitals concerned (relay with the “Care in Switzerland” program).
When a child is taken into care, his or her medical and social follow-up continues in his or her place of residence for as long as the situation requires. Once the child has recovered, we ensure that he or she can attend school or take a vocational training course.
Faits & Chiffres
Facts and figures of the Blind Driving Kids program in 2020
1987, program opened
In 2020
- 48 families have been followed in Mbour, Kaolack and Fatick, that is to say, 165 children
- 120 children in school
- 15 young people in vocational training
- 23 children too young to follow the school curriculum.
Facts and figures on the actions of the Talibé Children program in 2020
1987, opening of the program. Sentinelles has rescued XXX children
In 2020
- 6 daaras in Mbour have been monitored for health, social and educational needs
- 420 talibés received social follow-up, medical consultations and care when necessary
- 240 talibés have followed a school curriculum or literacy courses
- 6 talibés outside the daara benefited from social and/or medical follow-up and/or a return to their families.
Facts and figures on the 2020 actions of the Child Care program
In 2020
- 54 children suffering from various pathologies or after-effects of accidents followed
- Surgical mission with the University Hospital of Geneva (HUG) and the AEMV, in collaboration with the Hospital A. Le Dantec Hospital, for a plastic surgery for 2 young girls aged 14 and 15 years with severe burns after-effects and surgery for 2 women with tumors
- 1 woman with a maxillofacial tumor benefited́ from a transfer to Switzerland and a surgical intervention
- 1 Guinean child received surgery following trauma to her left eye; she also received a prosthesis.
Working teams
In Senegal: 8 local collaborators
- 1 expatriate delegate
- 4 social assistants
- 1 accounting secretary
- 2 guards
In Lausanne :
- 1 program manager at 60%.
Expenses in 2020: CHF 221,743
Our Partners
- Future of the child
- Center for the disabled of Mbour
- Handisable
- RADDHO (African Meeting for the Defense of Human Rights)
- AEMO (Action éducative en milieu ouvert), Mbour
- Marple Afrique Solidarité́, Saly
- CPRS (Center for promotion and social reintegration), Mbour
- Center for the Blind of Mbour
Switzerland

Care for children programme in Switzerland
The main disease treated in this programme is noma (see Noma Programme). In addition to causing the death of approximately 80% of the children affected, noma causes significant functional, aesthetic and psychological aftereffects and, when the disease has caused severe aftereffects, requires surgical treatment to enable children to have a well-proportioned face again.
The reconstructive surgery that allows children’s faces to be recreated includes plastic, reconstructive and aesthetic surgery, as well as maxillofacial surgery. This treatment requires considerable technical and human resources and, depending on the nature and severity of the aftereffects, cannot be carried out in the child’s country of origin. In such cases, the child is transferred to Switzerland to receive the treatment to which he or she is entitled.
Noma is the main disease requiring a transfer but, in rare cases, other diseases may be treated in this way (tumours, for example)
Faits & Chiffres
Care in Switzerland
Opening of the program in 1990.
Facts and Figures in 2020 of the “Care in Switzerland” program
Sentinelles rescued 8 children, including:
Surgical Component
Transfers to Switzerland:
- 8 patients, 5 of whom were already present in 2019, stayed in Switzerland at the Terre des hommes “House” in Massongex. Of the 8 patients, 2 are adults. 2 returned for the second and respectively the fourth time, after a first stay as a child.
- 17 interventions were carried out this year in Switzerland for a total of 156 days of hospitalization
- 6 days of hospitalization in the quarantine hospital Riviera-Chablais
- 5 children who arrived last year continued their treatment during this year
- 3 new patients were transferred to Switzerland during this year for treatment
- 6 patients returned home this year after their operation
- 93 medical consultations were carried out on an outpatient basis in the various hospitals
- 1319 days of accommodation at “la Maison” in Massongex
- 7 convoys were carried out by ASF
- 6 patients were seen for dental consultations before their return home
The suspension of operations at the University Hospitals of Geneva and of commercial flights has resulted in a significant decrease in the number of transfers and the extension of stays at the Terre des Hommes Valais reception center in Massongex
Working teams
In Lausanne:
- 1 program manager at 50%.
Expenses in 2020: CHF 59’463
Our Partners
- HUG
- TDH Lausanne
- TDH Valais
- Hôpital de Rennaz
- ASF
- Hilfaction
- Noma Hilfe